
We asked DMI whether they knew of existing models to link a certain increase in handwashing (say) with an impact on r or the reproduction number. They did not know of any such models, and we are also unaware of any. This makes it harder for us to build a cost-effectiveness model. At time of writing we do not have a cost-effectiveness model of DMI’s COVID-19-related work.
A counterargument against work in the development world is around whether flattening the curve is realistic in that context. Flattening the curve refers to controlling the spread of the pandemic so that it becomes manageable for the health system.
There have been question marks over whether it’s realistic to control the spread of the pandemic enough to stay within the capacity of the health systems in the developed world. It seems even more likely therefore that the health systems in the developing world will be overwhelmed, and therefore that any effort employed here will have no effect.
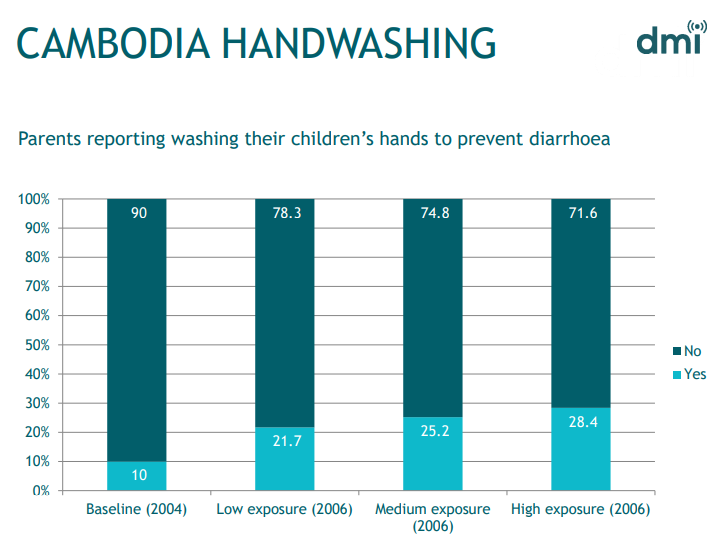
This concern seems all the more reasonable given that DMI’s past record on handwashing suggests that they can bring about an improvement, but it’s unclear whether they can bring about a drastic improvement (note that the context of a widespread, high-profile pandemic may invalidate our attempts to extrapolate from their past experience).
In discussion with DMI it became clear that the benefits go beyond lives saved from handwashing or (if applicable) social isolation. It includes, for example, tackling the risks of misinformation. For example in an environment with pre-existing ethnic tensions, rumours may spread suggesting that the virus was brought about by (e.g.) another racial group, which may exacerbate conflict risk, at a time when the world can least cope with large refugee camps or strains on health systems.
Our confidence in our tentative recommendation of DMI would be higher if we had the data and capacity to put together a model which reflects these factors.
Appendix: Biosecurity initiative at Centre for International Security and Cooperation
The Biosecurity Initiative at the Center for International Security and Cooperation (CISAC) is a research centre at Stanford that carries out policy research and industry outreach to reduce the risk of natural and engineered pandemics
Our recommendation of the Biosecurity Initiative of CISAC is based largely on the recommendation by Founders Pledge, set out in their report on existential risk. Their recommendation reflects the fact that their in-house biosecurity experts David Relman and Megan Palmer are both thought leaders in their field.
Our currently cursory review of their work suggests that their work is not very focused on COVID-19.
Appendix: Future of Humanity Institute (FHI)
FHI is a multidisciplinary research institute at Oxford University studying big picture questions for human civilization.
FHI has been funded in the past by the Open Philanthropy Project. We are familiar with work performed by a number of the thought leaders at FHI. We understand that FHI’s work mostly has little direct relevance to COVID-19, but some of it is relevant to pandemics.
Prior to the COVID-19 outbreak we reviewed FHI and deprioritised it because it was our impression that funding was not a particular constraint for FHI. Therefore, based on our current impressions, we are keeping FHI in the “not funding-constrained” category. Otherwise, it would likely fit well in the “co-benefits” category, because it does plenty of other work relevant to pandemics, bio risk, and funding directed to FHI may well funge with/enable other high-impact work.
Appendix: CSER (Centre for Study of Existential Risk)
The Centre for the Study of Existential Risk (CSER) is a research centre at the University of Cambridge, intended to study possible extinction-level threats
Our opinion that CSER is a high-impact donation target is supported by our view that (a) tackling existential risk a high-impact cause area (b) having this resource available in Cambridge is a solidly valuable thing. We understand that CSER’s work mostly has little direct relevance to COVID-19, but some of it is relevant to pandemics and that they are looking to expand this element of their team.
We believe that this may be a suitable choice for funders inspired to support pandemics as a result of the coronavirus outbreak.
Appendix: Work on Wet markets
Tackling wet markets has a clear link with COVID-19, since this is thought to be where the COVID-19 epidemic came from. Furthermore, multiple epidemics (avian flu and SARS as well as COVID-19) are thought to have originated in wet markets, because keeping live animals there increases the risk of zoonotic transmission. Tackling this issue has a number of co-benefits, notably for animals, who, we understand, suffer considerably as a result of these markets. Putting this area of work into a category which we are positive may suggest that we are positive about funding this area of work. However further work would be needed before we can conclude this.
A rough model for the impact of work on wet markets considers:
- The amount currently spent by governments and NGOs on this currently
- The scale of the impact of wet markets in terms of epidemic risk
- The scale of the impact of wet markets in terms of animal welfare
- We would need a fuller review to know how much is currently spent on this topic, however roughly extrapolating from what we know of the landscape, our rough guess is that the amount spent globally is fairly low, maybe c.$10million (rough order of magnitude)
- We know of three epidemics thought to originate from wet markets in the last 20 years. A more careful model would require more time than we have for this quick review, so let’s assume that the epidemic risk is captured by assuming that a pandemic of the scale of COVID-19 will occur once every hundred years as a result of wet markets. The economic impact of the coronavirus pandemic is thought to be at least $1 trillion (source: UN). This suggests that it would be worthwhile to invest $10 billion of effort (i.e. c1000x more than the amount currently expended) to move from the historic level of risk to zero risk. (Note that, as set out below, we are probably no longer at the historic level of risk anyway)
- To give some idea of the scale of suffering, we understand that there are 20,000 wildlife farms in China and also that there were 20,000 wet markets that China closed in February 2020. It is unclear how many animals would be on a farm or would come through a wet market per year, however if we assume that a moderately high estimate is 10,000 animals per farm, then this is c 200 million animals per farm. This is relatively small compared to the scale of industrial factory farming (e.g. c 60 billion factory farmed chickens). However, assuming that non-human animals are given sufficiently high moral weight, this scale is still sufficient to add a material amount of extra benefit to the work on wet markets.
While the above initial assessment sounds promising, we would need to further consider the following factors
- whether most of the work that needs to be done has already been done, given that China has recently banned wet markets and 80% of people in Beijing are opposed to wildlife meat markets
- it is reported that wet markets still persist, but to what extent is this the case?
- might control measures may drive wet markets underground in a way that might not be net beneficial
- might the ban spawn the creation of new wet markets in nearby countries
- is this area of work likely to be crowded as a result of COVID-19
- a full model of the impact of work on wet markets should consider what impact (if any) there will be on Chinese people’s nutrition as a result of the ban, as well as the animal welfare impact and the risk of epidemics.
We know of several organisations which we understand to be working on this:
- Wildlife Conservation Society
- Wildaid
- WWF
- EIA
- Traffic
- Flora and Fauna International
Appendix: Long list of COVID-19 related donation opportunities
A list of options
- Future of Humanity Institute (FHI)
- a multidisciplinary research institute at Oxford University studying big picture questions, includes a section on bio risks, including pandemics
- Centre for the Study of Existential Risk (CSER)
- a research centre at the University of Cambridge, intended to study possible extinction-level threats, including pandemics
- Johns Hopkins Centre for Health Security
- a think tank at Johns Hopkins University which carries out research on biosecurity and maintains a COVID-19 resource centre
- Biosecurity initiative at Centre for International Security and Cooperation
- a research centre at Stanford that carries out policy research and industry outreach; has general relevance to pandemics
- Tackling wet markets (multiple orgs)
- Wildlife Conservation Society
- Wildaid
- WWF
- EIA
- Traffic
- Flora and Fauna International
- WHO solidarity response fund: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/donate
- Send essential supplies such as personal protective equipment to frontline health workers
- Enable all countries to track and detect the disease by boosting laboratory capacity through training and equipment.
- Ensure health workers and communities everywhere have access to the latest science-based information to protect themselves, prevent infection and care for those in need.
- Accelerate efforts to fast-track the discovery and development of lifesaving vaccines, diagnostics and treatments
- Direct relief: https://www.directrelief.org/emergency/coronavirus-outbreak/
- provide personal protective equipment and essential medical items to health workers responding to coronavirus (COVID-19)
- Unicef: https://www.unicef.org.uk/donate/coronavirus/
- personal protection for health workers; hygiene materials for thousands of schools, public health facilities and other public places; and support with health education messaging
- Global Giving fund: https://www.globalgiving.org/projects/coronavirus-relief-fund/#menu
- We found no information whatsoever about how the money will be used
- Canadian Red Cross: https://donate.redcross.ca/page/55441/donate/1?locale=en-CA
- When we launch an appeal, donations made in response to it are used to help individuals and communities identified in the appeal recover from emergencies and disasters
- CDC foundation: https://www.cdcfoundation.org/
- This was listed as a coronavirus-relevant donation opportunity, however we have not found any coronavirus-relevant info on their webpage
- Southern Smoke Foundation https://southernsmoke.org/support/
- Help support those in the food and drink industry in crisis
- Italian ICU gofundme campaign https://www.gofundme.com/f/coronavirus-terapia-intensiva
- Funding ventilators and monitors etc for Ospedale San Raffaele di Milano
- First book: https://firstbook.org/
- First book aims to deliver 6 million books to kids in light of school closures
- Development Media International
- Project in Mozambique and Malawi (and possibly other countries) to promote handwashing and other relevant behaviours
- Univursa health
- They are looking to build a diagnostic support tool to help countries to rapidly identify possible outbreaks of COVID-19 within their borders, where those countries have limited capacity to do laboratory-based testing. There is a particular focus on sub-Saharan Africa.